Zika virus linked to stillbirth, loss of brain tissue
In January came the first case associating Zika virus to damage outside the central nervous system. An infected Brazilian woman gave birth to a stillborn baby with signs of severe tissue swelling and central nervous system defects causing near total brain loss.
This case gives evidence that not just microcephaly — the condition of an abnormally small head in newborns and widely linked to the Zika outbreak in Brazil — the Zika infection may also be linked to hydrops fetalis (abnormal accumulation of fluid in fetal compartments), hydranencephaly (almost complete loss of brain tissue), and fetal demise (stillbirth).
 WHO emergency response to Zika outbreak. WHO emergency response to Zika outbreak.
Researchers led by Albert Ko, MD at the Yale School of Public Health (YSPH) and Dr. Antônio Raimundo de Almeida at the Hospital Geral Roberto Santos in Salvador, Brazil — describe this case in the journal PLOS Neglected Tropical Diseases.
Researchers added that it is not possible to extend the application from this single case to all women exposed to ZIKA during pregnancy.
"These findings raise concerns that the virus may cause severe damage to fetuses leading to stillbirths and may be associated with effects other than those seen in the central nervous system. Additional work is needed to understand if this is an isolated finding and to confirm whether Zika virus can actually cause hydrops fetalis," said Ko, chair of the Department of Epidemiology of Microbial Diseases at YSPH, who has worked on the Zika outbreak in the coastal city of Salvador with Brazilian colleagues since shortly after the first cases of the mosquito-borne virus were reported there in early 2015.
The patient, a 20-year-old woman, was having a normal pregnancy during her first trimester. This changed abruptly during her 18th week of pregnancy, when an ultrasound examination discovered that the fetus' weight was well below where it should have been at that point.
The woman did not report any symptoms (rash, fever, or body aches) commonly associated with Zika prior to or during the early stages of her pregnancy. She also did not exhibit symptoms of other mosquito-borne diseases, including dengue or chikungunya. However, by her 30th week of the pregnancy her fetus showed birth defects. Labor was induced at the 32nd week.
Researchers subsequently confirmed the presence of the Zika virus in the fetus. The strain of Zika found appears to be the same strain currently spreading elsewhere.
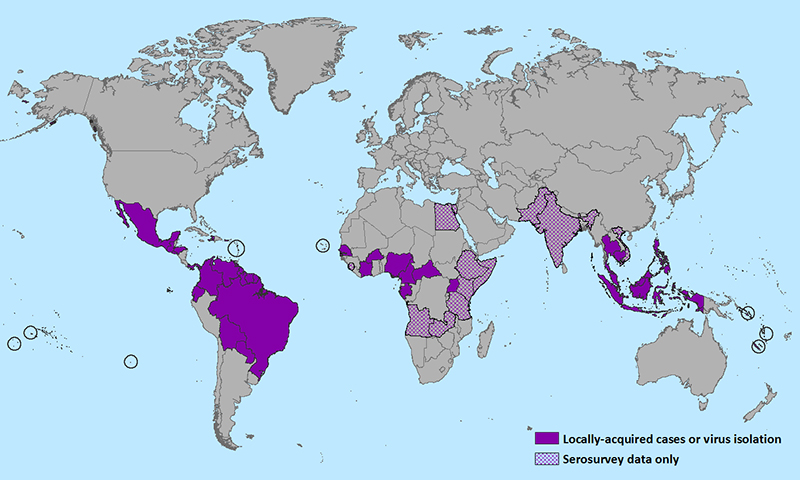
Since Zika appeared in Brazil, the virus has spread rapidly throughout much of Latin America and into the Caribbean. Several cases are also confirmed in the USA.
Researchers believe it is likely large numbers of pregnant women in Brazil and beyond will be exposed to the same Zika strain as the woman in this particular case, therefore further investigations are needed to determine risk of stillbirth and other adverse outcomes.
Ko worked with colleagues from the Hospital Geral Roberto Santos in Salvador, the Universidade Federal da Bahia in Salvador, the Oswaldo Cruz Foundation in Salvador, and the University of Texas Medical Branch in Galveston.
Abstract Background
The rapid spread of Zika virus in the Americas and current outbreak of microcephaly in Brazil has raised attention to the possible deleterious effects that the virus may have on fetuses.
Methodology/Principal Findings
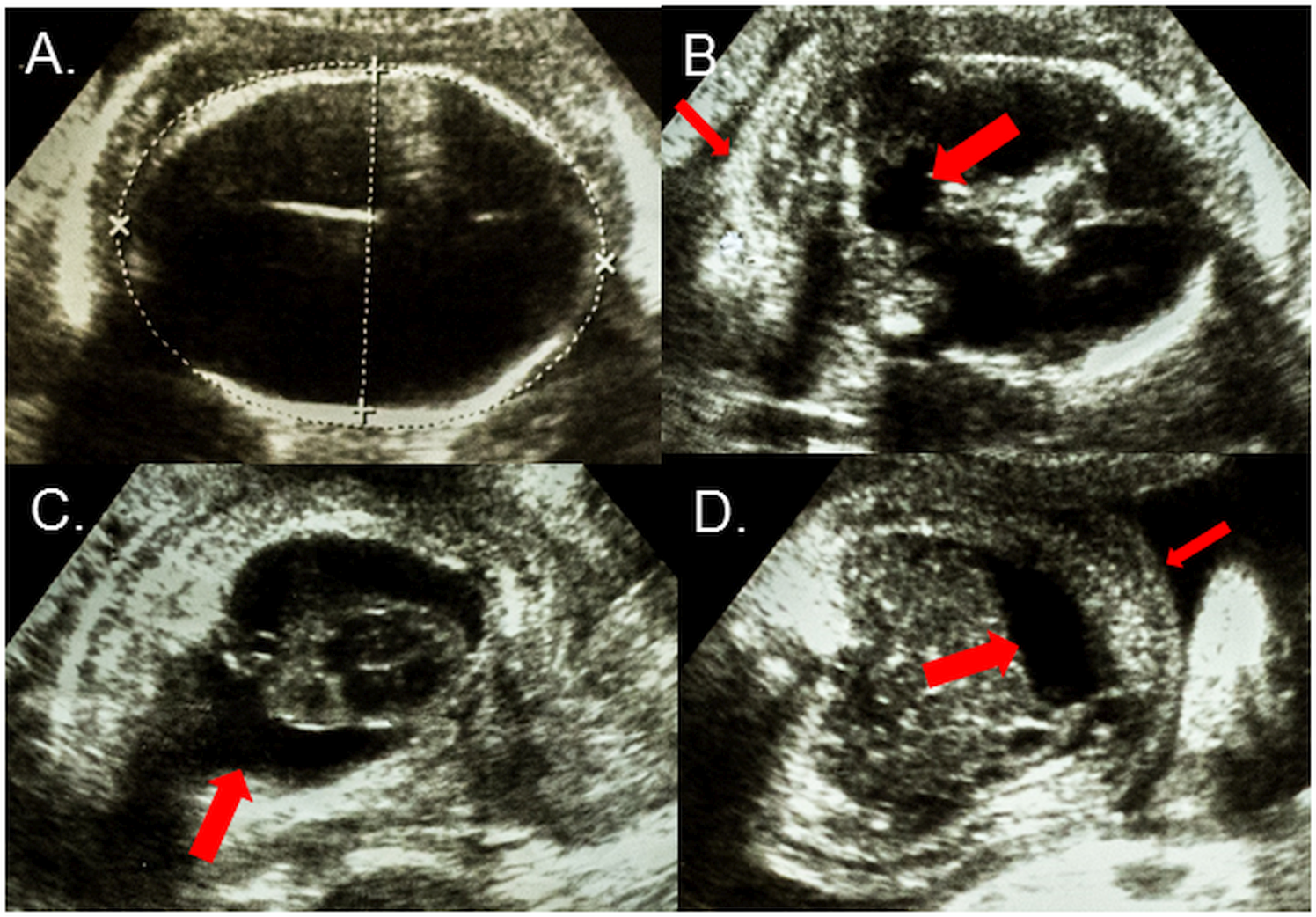
We report a case of a 20-year-old pregnant woman who was referred to our service after a large Zika virus outbreak in the city of Salvador, Brazil with an ultrasound examination that showed intrauterine growth retardation of the fetus at the 18th gestational week. Ultrasound examinations in the 2nd and 3rd trimesters demonstrated severe microcephaly, hydranencephaly, intracranial calcifications and destructive lesions of posterior fossa, in addition to hydrothorax, ascites and subcutaneous edema. An induced labor was performed at the 32nd gestational week due to fetal demise and delivered a female fetus. ZIKV-specific real-time polymerase chain reaction amplification products were obtained from extracts of cerebral cortex, medulla oblongata and cerebrospinal and amniotic fluid, while extracts of heart, lung, liver, vitreous body of the eye and placenta did not yield detectable products.
Conclusions/Significance
This case report provides evidence that in addition to microcephaly, there may be a link between Zika virus infection and hydrops fetalis and fetal demise. Given the recent spread of the virus, systematic investigation of spontaneous abortions and stillbirths may be warranted to evaluate the risk that ZIKV infection imparts on these outcomes.
Author Summary
The rapid spread of Zika virus in the Americas and outbreak of microcephaly in Brazil has raised attention to the possible deleterious effects that the virus may have on fetuses. We report a case of a 20-year-old pregnant woman from Salvador, Brazil whose fetus had developed hydrops fetalis, a condition where there is abnormal accumulation of fluid in the fetus, as well as severe central nervous system defects such as microcephaly and hydranencephaly. After fetal demise, ZIKV RNA was detected in central nervous system tissues and amniotic fluid. The case report provides evidence that in addition to microcephaly, there may be a link between Zika virus infection and hydrops fetalis and fetal demise. Given the recent spread of the virus, systematic investigation of spontaneous abortions and stillbirths may be warranted to evaluate the risk that ZIKV infection imparts on these outcomes.
Return to top of page
|